Introduction
Secondary hypertension is incredibly common.
This is an undervalued area in general practice. The most common thing I see occur is we keep stacking on antihypertensives and treat the number to reduce the risk of cardiovascular disease. However, we often forget to ask the question, “Is there an underlying cause here?”
The purpose of this post is to get people thinking about secondary hypertension and flagging it early on top of guidance for Conn’s/primary hyperaldosteronism evaluation. We in general practice are able to identify these individuals with secondary hypertension and therefore provide the care required to reduce their risk of cardiovascular disease.
Incidence of secondary causes of hypertension
1 in 10 patients with hypertension have a secondary cause.
The most common presenting complaint in general practice is hypertension based on the BEACH data – 5.7% of problems encountered and 9 out of 100 encounters). I think we underappreciate these numbers.
The following factors make it even more likely a secondary cause is at play
- Onset less than 40 years old
- Abrupt onset
- Abrupt worsening despite previously good control
- Hypertensive urgency or emergency
- Resistant hypertension (3 agents with diuretic = uncontrolled OR 4 or more agents needed)
- Target organ damage that is disproportionate
- Family history
- Clinical clues – hypoK, SeCr >20% rise post ACEI/ARB, or paroxysmal HTN
In terms of prevalence in unselected hypertensive patients we need to think of the big 3
- Obstructive sleep apnoea – 25%
- Sleep study
- Primary hyperaldosteronism – estimates range from 5 to 15%
- Renin-aldosterone ratio in the setting of withholding medications that interfere with it’s measurement
- Renovascular disease – 5% (parenchymal is much less at 1%)
- renal function test combined with urine microalb:cr ratio with a urine MC&S
The clinical literature highlights that testing for these conditions first is reasonable given the incidence of them being the highest
Don’t forget the medications we throw patients on: SNRIs, stimulants, NSAIDs, COCP, nicotine, alcohol and more.
For other rare disorders we ought to be guided by the clinical picture which includes: Cushing’s syndrome (<1%), pheochromocytoma (<1%), aortic coarctation (<1%).
Several other rare causes are out there… such as the potassium wasting disorders. But I digress. Heck even licorice apparently in excess can cause hypertension.
So… I want to test for primary hyperaldosteronism – how do I do it?
Firstly, don’t do it if the risk of having uncontrolled hypertension in the 160s or more is likely to occur.
If we have a patient who we are confident we can do it for the Endocrine Society provide an excellent guide for testing that was formulated by the Endocrine Hypertension team at Hudson Institute of Medical Research. We need to do the aldosterone-renin ratio test.
You can find their amazing document here: https://www.endocrinesociety.org.au/New%20Resource.pdf
This table encapsulates the medications that interfere with the ARR
| Causes of false positive ARR | Causes of false negative ARR |
| β-blocker (e.g. metoprolol, atenolol) α-methyldopa Clonidine | Diuretic (e.g. hydrochlorothiazide, frusemide, indapamide) MR antagonist (e.g. spironolactone, eplerenone) ACE inhibitor (e.g. perindopril, ramipril) Angiotensin II receptor blocker (e.g. irbesartan, telmisartan) Dihydropyridine calcium channel blocker (e.g. amlodipine, lercanidipine) |
Basic rule to withhold: diuretics (including MRAs) 6 weeks and everything else 2 weeks.
Then the testing can occur. Another really important aspect of it is making sure the patient’s potassium is greater than 4.0 – therefore replace it with slow K or chlorvescent.
The medications used to hold a person’s blood pressure under control are:
| Medication | Dose | Initiation |
| Verapamil SR | 180-240mg BD | 90mg-180mg daily |
| Prazosin | 0.5mg-5mg BD or TDS | 0.5mg BD |
| Moxonidine | 200-400microg daily | 200microg nocte |
| Hydralazine | 12.5-50mg BD | 12.5mg BD |
Hydralazine can go up to 300mg per day – however over 200mg is asking for trouble. Beyond 200mg, 1 in 10 patients can get hydralazine-induced lupus-like syndrome which can be delayed.
I often find verapamil with prazosin first is the combination I’m favouring – prazosin sometimes can induce tachycardia and verapamil offsets it.
I also give a fact sheet for patients because the following things need to occur
- The patient must have a medication management plan as above with the GP or specialist
- The patient must stop any NSAIDs
- The patient cannot eat liquorice for at least 1 week before the test
- The patient must be out of bed for at least 2 hours
- The patient must be seated 5-15mins before the test
This is the factsheet I give: https://www.sapathology.sa.gov.au/assets/downloads/Patient-information/PUB-0837.pdf
The ARR
It’s unfortunately a screening test. The variation in renin levels, aldosterone levels and other biological factors make so it can be challenging. A study looking at 7150 participants in a meta-analysis shows that the pooled sensitivty was 81.6% and specificity was 93.3%. Therefore further testing is always warranted
The saline suppression test is the next step of care requiring the endocrinologist’s expertise.
The pathway looks like this generally:
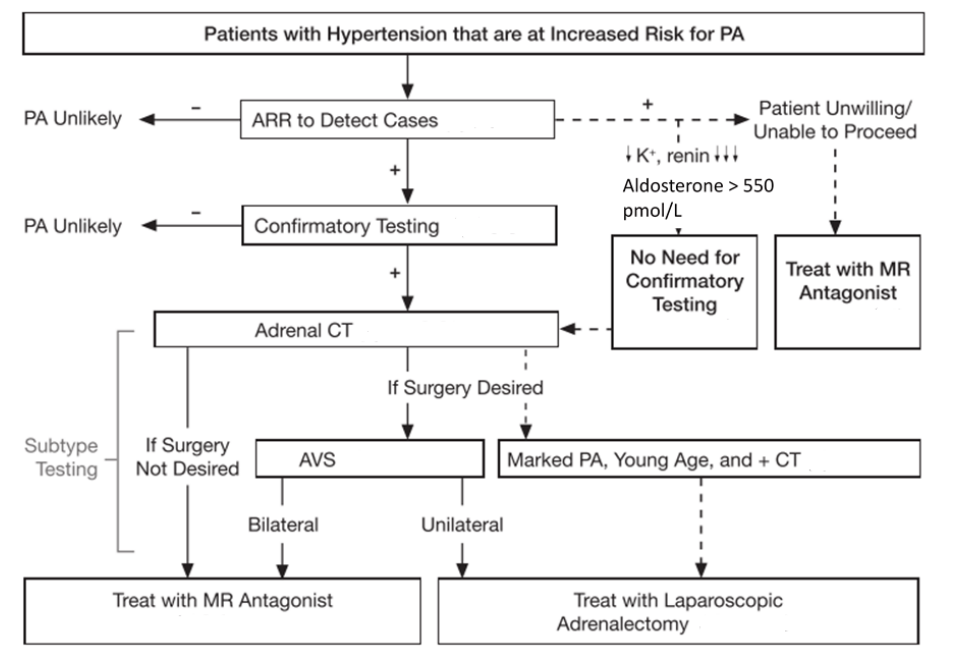
I have to say this summary from the Endocrine Society in their giant guide has been incredibly handy for me – you can find it in the HEDTA manual: https://endocrinesociety.org.au/downloads/20230131%20MASTER%20Harmonisation%20of%20Endocrine%20Dynamic%20Testing%201.9.pdf
I’ve had patients who do not wish to proceed with further testing at all. Having this knowledge to highlight to them what they would be in for if we discuss this pathway is really important for informed consent. I have a few patients with positive ARRs with hypertension in the 180s and 190s on three agents and then I introduce spironolactone where I titrate it to 200mg or more which leads to normotension and the removal of all of their agents.
Conclusion
Key points to remember are:
- 1 in 10 individuals with hypertension on average have a secondary cause
- Secondary causes are more likely with certain factors – abrupt onset, <40y.o, hypertensive urgency/emergency, family history
- Most common secondary cause is OSA > primary hyperaldosteronism > renovascular
- Think about the clinical picture before diving into testing for cushing’s, pheo, coarctation and other rare causes
- Primary hyperaldosteronism testing requires
- Withholding medications – diuretics/MRA 6 weeks, ACEI/ARB/beta-blockers/DCCBs 2 weeks
- Transition to antihypertensives: verapamil SR + prazosin first >> moxonidine > hydralazine
- Testing with ARR – beware of the sensitivity being ~80%
- Patients can decline to go onwards to saline suppression test / surgical intervention and it would be appropriate to manage with spironolactone (which can go up to 300mg PO daily)
References
Chiang C, Inder W, Grossmann M, Clifton-Bligh R, Coates P, Lim EM, et al. Harmonisation of Endocrine Dynamic Testing – Adult (HEDTA) [Internet]. Australia: Endocrine Society of Australia and Australasian Association of Clinical Biochemists; 2021 [cited 2026 May 9]. Available from: https://endocrinesociety.org.au/downloads/20230131%20MASTER%20Harmonisation%20of%20Endocrine%20Dynamic%20Testing%201.9.pdf
Funder JW, Carey RM, Mantero F, Murad MH, Reincke M, Shibata H, et al. The management of primary aldosteronism: case detection, diagnosis, and treatment: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2016;101(5):1889-1916. doi:10.1210/jc.2015-4061
Kao TW, Chen JY, Liu JH, Tseng WH, Hsieh CC, Wu VC, et al. Diagnostic efficacy of aldosterone-to-renin ratio to screen primary aldosteronism in hypertension: a systemic review and meta-analysis. Ther Adv Endocrinol Metab. 2024;15:20420188241303429. doi:10.1177/20420188241303429
Siru R, Conradie JH, Gillett MJ, Page MM. Approach to the diagnosis of secondary hypertension in adults. Aust Prescr. 2021;44:165-9. doi:10.18773/austprescr.2021.038

Leave a comment