Introduction
In General Practice we likely overdo it with antibiotic prescriptions in the setting of respiratory tract infections. There is more and more data to demonstrate that we actually do more harm to the patient providing antibiotics for respiratory tract infections and other common presentations to the General Practice. This is a combination of not only the potential adverse events that can occur but also increasing antimicrobial resistance is escalating all over the world where mult-resistant microbes are bullet proof against our arsenal of antimicrobials.
This post will be focused on looking at the evidence behind antibiotic use for patients presenting with a sore throat, what the benefits and harms are, and what strategies we can use as GP to reduce antibiotic use in non-indicated circumstances.
The sore throat
I’m going to be looking at Cochrane reviews for this one. Published in 2021, ‘Antibiotics for treatment of sore throat in children and adults’.
You can find it here: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD000023.pub5/full?highlightAbstract=antibiot%7Cantibiotics
I think the Cochrane reviews are great. I think they provide reviews of the literature and provide robust, non-biased and informative deductions. This one looked at 15,337 cases from a total of 29 trials. A weakness of these studies of course is the majority of them took place in 1950, the sample size was insufficient to see if antibiotics reduced glomerulonephritis. It is worth noting that a reduction in symptom duration was sufficient: the number needed to treat to prevent 1 sore throat at day three was less than 6 and at one week it was 18. It certainly did reduce acute otitis media and quinsies within 2 months as well.
I hold a similar opinion to the conclusions of the author: we have to judge on an individual basis if there is likely a bacterial cause, balance the modest symptom reduction with antimicrobial resistance.
We know the two most common causes of sore throat are viral pharyngitis and viral tonsillitis. Another interesting study from the FRACGP (https://www1.racgp.org.au/ajgp/2018/july/sore-throat-in-primary-care) looked at the attitude we have towards sore throats. It’s really fascinating to see we still continue to push antibiotics for concerns around bacterial (specifically group A Streptococcus).
The current evidence through Therapeutic Guidelines, where they use quite robust reasoning and references, indicate that for patients without high risk of rheumatic heart disease in Australia routinely do not require antibiotics even if they have Group A Strep. There is limited evidence to suggest prevention of glomerulonephritis in the future. At best, we can reduce the symptoms of the illness by 1 day – but then all the risks of antibiotics come on board.
I always offer symptomatic management strategies with this little handout: https://www.nps.org.au/assets/fc2723c4a3fcdec8-31e4936adc6c-NPS-MedicineWise-RTI-Action-Plan-1.pdf
Trying to reduce antibiotic use for sore throats
So the conclusion should be we should try to stop ourselves prescribing antibiotics in these circumstances where the patient is not high risk of acute rheumatic fever. Of course, if there is Scarlet Fever which then changes the approach. However, there’s no concrete evidence to show that antibiotics prevent scarlet fever but it does need 10 days of antibiotics to treat if present.
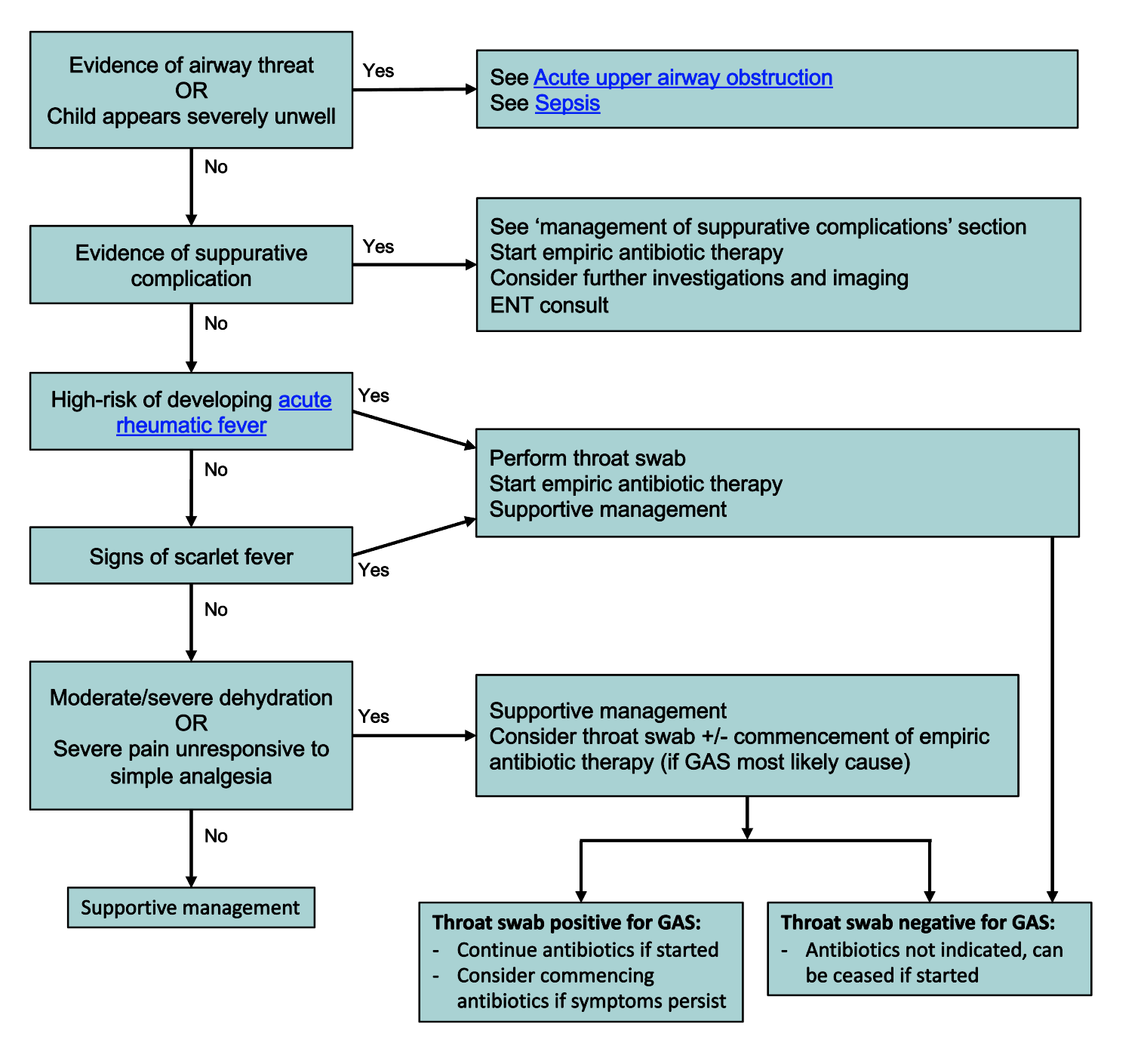
The Royal Children’s Hospital hold a similar view and we should hold off on antibiotics for children presenting with a sore throat without red flags. And I quote, “Group A streptococcus (GAS) is the most frequently implicated bacterial pathogen. It is usually self-limiting, difficult to distinguish from viral infection and empiric antibiotic therapy is not required for most patients”
The information chart I like using to inform patients is from the RCH itself: https://www.rch.org.au/uploadedImages/Main/Content/clinicalguide/guideline_index/Sore-throat-management.png
The other information sheet I like to use is: https://www.safetyandquality.gov.au/sites/default/files/2024-03/Patient-Decision-Aid-Sore-Throat_0.pdf
These tools help the reduction on antibiotic prescriptions.
But what if parents insist? What do we do then? What if you’re not stern and easily cave in to demands?
Two great articles to read:
https://www1.racgp.org.au/ajgp/2022/january-february/reducing-antibiotic-prescribing-with-patients
https://www.racgp.org.au/afp/2016/september/is-australia-ready-to-implement-delayed-prescribin
Delayed antibiotic prescribing works! It reduces antibiotic use. It lets you keep rapport. It’s part of shared decision making – which is what we’re all about. Give the patient all the information we have above and let them weigh up the pros and cons. Although, I have to admit, I have been quite stern at times and refuse it outright because we also have a duty of care to the wider community with regards to antibiotic resistance for the future.
Another part of the care process we do not often highlight enough here as well is acknowledging parental concern and they worry for their kid. Highlighting that you want to do the right thing by their child too, and that you know they want their kid to get better and improve quickly so they’re not suffering. You don’t want to cause more problems with side effects because you know parents worry about that too. These make us less appear less cold and calculating.
Conclusion
Shared decision making and providing the data plus facts for patients is the way to go. If we want to reduce antibiotic prescribing we need to spend more time educating our patients about the benefits and harms of antibiotics so that they can make an informed decision about their care or their child’s care.

{kind=link}
Leave a comment