Introduction
Apolipoprotein B (ApoB) has emerging evidence as the marker to predict the risk of cardiovascular disease for primary prevention. Systematic reviews and meta-analyses released in the last few years demonstrate it is a valuable tool we can use in Australian General Practice.
At this stage, the General Practice in Australia has not yet adapted it into routine clinical practice. I anticipate this will change in the next few years. At the moment the test is private but I do think that it will potentially become medicare-rebatable. The question then remains is when would it be indicated: is it going to fall into the recommendation of using it alongside total cholesterol to HDL ratio for risk stratification in the AusCVDRisk calculator, or is it going to be indicated in select circumstances?
This post will explore the basic pathophysiology behind ApoB, review the meta-analyses out there and formulating what I think how ApoB will be used for primary prevention based on the evidence presented.
Basic Pathophysiology and Lipid Profile Testing
Cholesterol is transported in the blood stream through he use of lipoproteins – this is because cholesterol is not hydrophilic (that is it will not dissolve in water) and the lipoproteins enable this dissolution. These lipoproteins include HDL, IDL LDL, VLDL, lipoprotein A and chylomicrons (which contain triglycerides). The size of these lipoproteins can vary – this is a very important point to remember for later when we talk about LDL, LDL-cholesterol and ApoB together.
ApoB is a lipoprotein that is synthesized by the liver. It is a protein that is attached onto these lipoproteins: specifically VLDL, IDL, LDL and lipoprotein A. It is important to note here HDL does not have ApoB at all. Each lipoprotein has a single ApoB attachment on it
What we know about ApoB is that it is very atherosclerotic in nature: the Journal of the American Heart Association published a review article encapsulating the mechanisms of how ApoB works in 2022 (https://doi.org/10.1161/JAHA.122.025858). ApoB loves to deposit itself and becomes trapped in the arterial walls – this is the key driver of atherosclerosis, not the lipoprotein itself. Increasing amount of ApoB particles in the blood stream proportionately increases the risk of cardiovascular disease.
Key message so far is more particles of lipoprotein (except HDL) in the plasma means more ApoB particles, which means increasing cardiovascular disease risk.
When we do a lipid profile, we get the following results: LDL-C, HDL-C, total cholesterol, TG and non-HDL cholesterol. The LDL-C is an indirect measurement based on the following formula:
LDL-C = Total Cholesterol – HDL-C – (Triglycerides / 2.2)
The triglyceride level is used to approximate the VLDL-C (triglycerides/2.2) level to get the LDL-C. The measurement here is mmol/L. Thus, escalating triglyceride levels means we cannot calculate the LDL. The equation can give us non-HDL totals by having TC – HDL-C levels (which becomes a combination of VLDL and LDL). So the LDL-C is an estimate – it’s not perfect. Then again, we are not using LDL-C anymore in our AusCVDRisk calculator and even then it’s a crude marker for “good” cholesterol versus “bad” cholesterol.
Imagine the following hypothetical. Person A has 10 cherries and each cherry weighted 0.5g. Compare that to person B who has 5 cherries that weight 1g. In both situations, you have a total weight of 5g but in the first instance there’s more cherries, meaning there’s 10 stems versus 5 stems.
Picture 1: cherries and stems – ApoB (stem) and LDL particles (cherries)
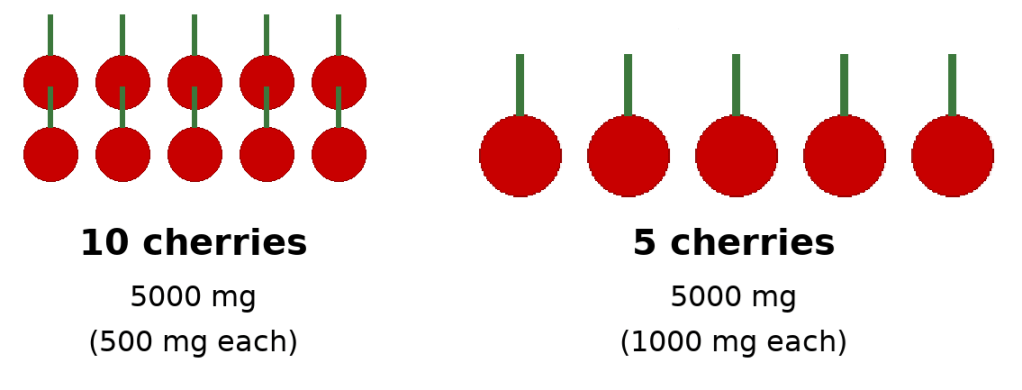
Using this perspective, each stem represents ApoB, and each cherry represents a LDL particle (remember each LDL particle can vary in size): although the total amount of weight of cherries (LDL-C) is the same in both situations, because the first situation has more LDL particles, and thus, more ApoB, the first situation has a higher atherosclerotic risk.
This there in lies the weakness of LDL-C as a measurement in how we do via the lipid profile: we get an indirect quantity of LDL-C and we can’t measure the number of LDL particles. This means we cannot measure ApoB which is the true driver of plaque deposition in the arterial wall. Using our prior model without ApoB, we would say the cardiovascular risk in both situations is the same. This is not correct and ApoB measuring is much more accurate.
The new testing we have available, with cost reducing over time, is a direct measurement of the ApoB molecule itself in the bloodstream – we can quantify the concentration (and thus the amount) therefore we can risk stratify better as we directly measure how many atherosclerotic cannonballs are out there.
ApoB and CVD risk stratification
Table 1: recent studies showing ApoB and it’s role in CVD primary prevention
| Study (Year) | Type of Study | Population / Sample Size | Key Findings | Relevance for Primary Prevention |
| Katsi V et al., 2025 The Role of Non-HDL Cholesterol and Apolipoprotein B in Risk Stratification and Therapeutic Targeting | Narrative review (biomarker foundations) | Population synthesis from multiple cohorts (>1 million individuals referenced across included studies) | ApoB & non-HDL-C outperform LDL-C across risk states, especially mixed dyslipidaemia & metabolic syndrome. | Shows ApoB’s superiority in real-world primary prevention settings where LDL-C underestimates risk. |
| Sehayek E et al., 2025, J Clin Lipidol ApoB, LDL-C & non-HDL-C discordance: Systematic Review & Meta-analysis | Systematic review (33 studies) | Total pooled population >500,000 individuals from primary & secondary prevention cohorts | ApoB is most accurate predictor when LDL-C/non-HDL-C discordant; treatment decisions should prioritise ApoB. | Key SR showing ApoB should guide therapy & risk categorisation in general practice. |
| De Oliveira-Gomes D et al., 2024, Circulation Apolipoprotein B: Bridging the Gap Between Evidence and Clinical Practice | Expert translational review | Synthesises data from trials, cohorts, & MR studies (>1.5 million total participants represented) | Provides practical ApoB cut-offs: <1.0 g/L primary; <0.8 g/L secondary. | Most clinically useful paper for how to incorporate ApoB into GP prevention workflows. |
| Sayed AH et al., 2024, JAMA Cardiol Discordantly Elevated ApoB in Adults With Normal LDL-C | Cross-sectional cohort study | 12,688 statin-naïve adults (NHANES) | 20–30% had high ApoB despite normal LDL-C; these individuals had higher predicted ASCVD risk. | Demonstrates how LDL-C misses risk → supports once-off ApoB for primary prevention. |
| Sniderman AD et al., 2024, Eur Heart J ApoB vs LDL-C Discordance in UK Biobank | Large prospective cohort | 293,876 adults, 11-year median follow-up | When discordant, risk follows ApoB, not LDL-C. | Excellent for reclassifying patients in intermediate ACVDR categories. |
| Yang J et al., 2023, JAMA Network Open Dose-response Mendelian Randomisation of Lipids | Mendelian-randomisation study | ~440,000 UK Biobank participants | ApoB has strongest causal relationship with CAD & mortality vs LDL-C or TG. | High-quality causal evidence → ApoB is the true biological driver of first ASCVD events. |
| Glavinovic T et al., 2022, J Am Heart Assoc Why ApoB Is Superior to LDL-C and non-HDL-C | Mechanistic + narrative evidence synthesis | Population mechanisms based on large cohort data (e.g., INTERHEART, UKBB; >200k represented) | Demonstrates physiologic basis: atherogenic particle number (ApoB) causes plaque, not LDL-C mass. | Helps explain to clinicians/patients why ApoB should be measured even with “good LDL-C.” |
| Khan SU et al., 2020, Eur J Prev Cardiol Systematic Review of RCTs: ApoB-lowering & CV Outcomes | Meta-analysis of 29 RCTs | ~333,000 participants | Every 10 mg/dL reduction in ApoB → 7–12% reduction in MACE. | Direct evidence that treating to lower ApoB improves outcomes. |
| Large population-level meta-analyses (pre-2020) (e.g., Emerging Risk Factors Collaboration analyses) | Systematic review/meta-regression | Cumulative population in hundreds of thousands | ApoB stronger predictor than LDL-C in multiple pooled cohorts. | Lays foundation behind ApoB’s adoption by cardiometabolic prevention groups. |
| Sniderman AD et al., 2019 Apolipoprotein B particles & ASCVD risk | Narrative review (expert synthesis) | Synthesises major datasets (>1 million across cited cohorts) | Early consolidation showing ApoB > LDL-C globally. | Background reference showing longstanding consistency of ApoB evidence. |
We can confidently say that the pathophysiological basis of atherosclerosis from ApoB is translated into the data we see repeated in the studies. I have provided a table that summaries key articles I have identified and the key messages to take away from them
What does that mean for us in general practice in Australia?
If we look at how the AusCVDRisk calculator works I suspect ApoB will help stratify further for thinking about life time risk as it’s role is to build plaque. The challenging thought is how is this going to be incorporated into the CVD risk calculator? It could potentially be the next step after the AusCVDRisk calculation and become the following
Table 1: ApoB concentration and using it to adjust AusCVDRisk %
| ApoB band | Apply multiplier to ACVDR % | Reason |
|---|---|---|
| <0.8 g/L | ACVDR × 0.7 | Lower observed events in low-ApoB phenotypes |
| 0.8–1.2 g/L | ACVDR × 1.0 | ACVDR fairly accurate |
| >1.2 g/L | ACVDR × 1.5–1.7 | HR ~1.4–1.75 consistently reported |
If we’re thinking relative to the CT calcium score scan, I think ApoB is better for thinking far in the future whereas the calcium score will let us know how much plaque there already thus guide us more definitively in the next few years.
There will be more nuance here I suspect once it rolls out in deciding what to do with the intermediate risk factors with the use of ApoB versus CT calcium scoring.
For patients who have statins commenced then the question becomes what should be measure? The data is pointing towards ApoB and depending on the risk patients are either going to be pushed to be <0.8 for those are high risk and <1.0 if in other risk categories. What we see is LDL declines in parallel with ApoB – not unsurprising given a LDL particle has an ApoB particle.
Summary
- ApoB is the way forward in measuring CVD risk for primary prevention and will guide management in the future
- ApoB itself is a direct promoter of atherosclerosis – it glues lipoproteins/cholesterol into the arterial walls causing plaque formation over time.
- Our current lipid profile testing is a crude estimate of “good” versus “bad” cholesterol providing a less precise estimate of a person’s CVD risk in the primary prevention setting.
- ApoB testing can directly calculate the particles circulating in a person’s blood stream via concentration of it and this can direct risk based stratification better
- Table 1 is what I suspect the future use of ApoB to be based on the clinical data.
- Future guidelines will likely advocate for ApoB < 0.8 for high risk individuals if treating with statins and <1.0 for the lower risk individuals.

Leave a comment